The First Sign of Crohn's Disease,
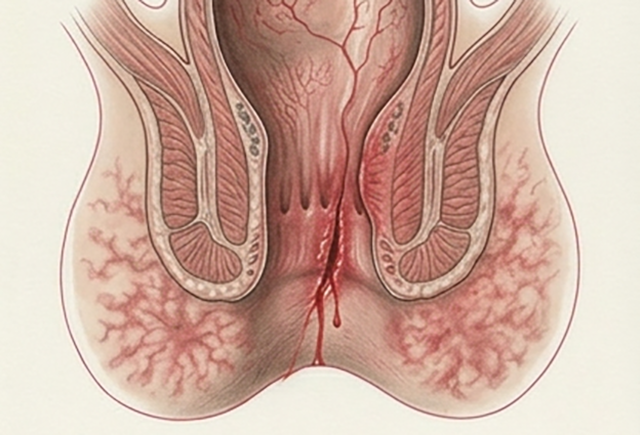
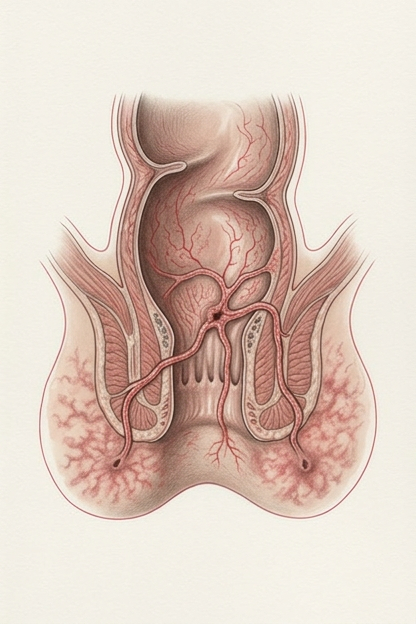
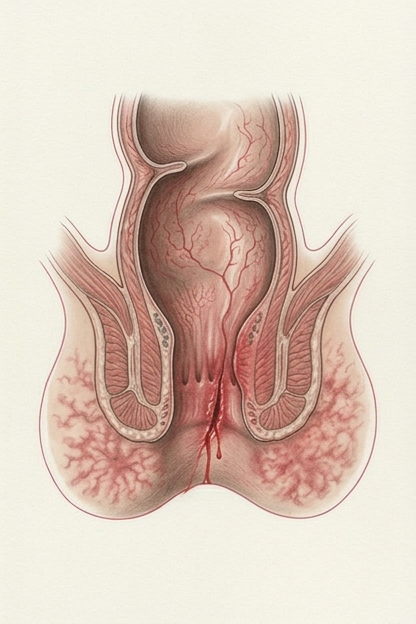
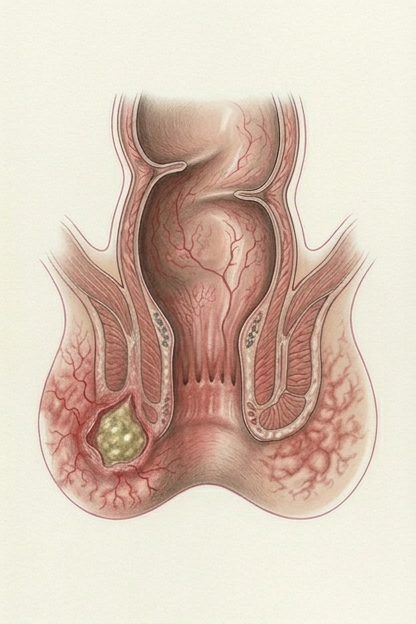
Anal Lesions
Perianal lesions can be the first sign of Crohn's disease in approximately 17.2% of all patients, appearing more than 6 months before the diagnosis itself. It is reported that fistulas occur in 10-26% of Crohn's patients worldwide, and complex fistulas are harder to treat compared to simple ones, with lower chances of Crohn's disease remission.
Cumulative Incidence of Perianal Disease
Within 1 year
12%
Within 5 years
15%
Within 10 years
21%
Within 20 years
26%
* The prevalence of fistula depends on the disease location: 12% for isolated ileal disease, 15% for ileocolonic disease, 41% for colonic disease, and it is most severe at 92% when the rectum is involved.